
The COVID pandemic has been overtaking our year, form rising cases, rising deaths, and rising unemployment rates, it’s clear that this pandemic affects all of us. Due to a variety of variables including limited healthcare, limited traveling, and not being able to leave our homes; there are going to be inevitable repercussions. Anxiety has remained steady in almost all of us, whether we are worried about finding a new job or going stir crazy trying to care for our children. However, there is one population other than the elderly extremely vulnerable to this virus and the environment this pandemic has created – those who regularly seek mental health treatment and addiction treatment.
Near Denver, Colorado, a woman named Sara Witter had relapsed in December. She attended a detox and treatment and started to get her life back in order. She was talking a monthly injection to block her cravings from opioids. During the next couple months, she was working for a local health association, advocating for substance abuse treatment, and even was engaged to be married.
This came to a halt when COVID hit.
Due to lockdown orders, her support systems vanished. She no longer was able to attend her NA meetings. No longer able to talk to her friend or her sponsor over coffee. To make matters worse, the hospitals became overworked and thus had to push back her injection shot from 30 days to 45 days.
By reconstructing her last days from her phone, her family was able to assess that Sara started using again a week after her injection appointment should have been. Her appointment was on Friday, but that Tuesday and Wednesday she continued to use to fend off the cravings.
Thursday, the day before her appointment, her sister came home to something no family member should ever see. Sara had overdosed (most likely from fentanyl) and was lying on her bed, syringe in hand and foam around her mouth.
Sadly enough, Sara’s story is just one of many. During 2018, (a normal year without COVID) there averaged 22.8 deaths per day in just Florida alone. Due to high-stress situations along with limited resources, this number is expected to climb during 2020.
People struggling with a substance use disorder, whether to opioids, alcohol, or any dangerous drug are hanging on by a thread. They rely on their healthy friendships, support, counseling, and, yes, medication to keep on the right path. Without these support systems and safety nets, where are they to turn?
The Problem With Reporting
Then rises the problem of accurate reporting. Sara Wittner’s case is just one example of how the COVID pandemic has caused a death, but will her death be tallied? Because she didn’t represent symptoms of COVID-19 around the time of her death, probably not; however this illustrates the complexity of tracking the full impact of the coronavirus pandemic.
Some individuals die from COVID-19. Others die from some other disorder, but test positive for the virus. And people like Sara Witter die from the environmental disruptions of the pandemic.
Public health officials are still trying to collect and analyze data from COVID tests and deaths, but the pandemic has left an untold number dying in the shadows, not directly because of the virus but still because of it.
But, even the numbers for COVID cases and deaths are a little blurry, so much in fact that conspirators on twitter and even the president have claimed the tallies to be exaggerated – even without the inclusion of indirect deaths like Sara. This idea has made it hard for health officials to establish infection prevention measures.
However, experts still believe that due to the lack of testing, lack of standards in reporting, and the effects of the social and economic disruption has still underreported the full extent of the death toll.
How Reporting is Done
In the U.S., because COVID-19 is a “notifiable disease”, doctors, coroners, hospitals, and nursing homes must report if someone has been infected and also when a person known to have the virus dies. This provides health officials real-time surveillance on the outbreak in an effort to provide relief and solutions in a timely manner. On the other hand, this system is designed for speed rather than accuracy. This type of reporting will inevitably report deaths not caused by the virus, while at the same time fail to report many of the deaths that were.
For instance, someone tested positive for COVID-19 may die from a car crash and be included in the COVID death toll. On the other hand, someone dying from home might not be counted if they were never tested. At this point in time, there is no way to know if we are currently under or over-reporting, but chances are the numbers are fairly close due to these variables.
The difficult part of this type of reporting is that COVID-19 deaths are not black and white. For instance, the Center for Disease Control and Prevention guidelines allow for doctors to attribute a death to a “presumed” or “probable” COVID infection in the absence of a positive test if the patient’s symptoms or circumstances warrant it. Doctors and coranors completing these reports rely on their own medical judgment, creating variations in reporting standards from state to state. Therefore, if someone dies in their home, but has symptoms, it is left up to the diagnosis of the coroner to decipher if the death was impacted by a virus without a positive test.
Making the situation more complex is the difference between people dying from COVID-19 and people dying with COVID-19. Clearly underlying disorders like hypertension, diabetes, and asthma can all impact how the virus affects an individual, but the cause of death could be different from one coroner/doctor to another.
For this reason, we must compartmentalize these deaths into separate categories.
- Those who died from COVID-19 alone
- People who’ve died from COVID and another co-occurring health condition
- Those who have died while presenting signs of COVID but test was done
- Individuals who have died while presenting signs and while also having another health condition
- And possibly indirect deaths like Sara who’ve died from the disrupted care of the pandemic.
Of course this reporting would take more effort and time, causing delayed reporting and thus might hinder rapid response from health organizations. Also, this reporting may not accurately depict the deaths away from hospitalized settings as bodies are not tested after death and therefore COVID deaths are often underreported in this way.
Utilizing Historical Data for Excess Deaths
For this reason, researchers are utilizing what is known as “excess deaths.” The public health system tracks deaths by county and can provide a good sense of the expected deaths for the year. The number above the expected baseline could provide the extent of the effects of the pandemic.
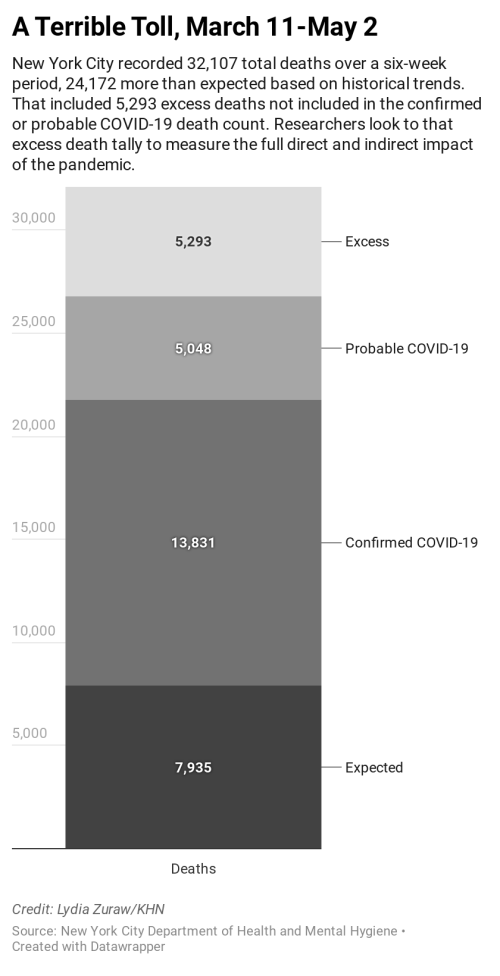
For example, from March 11 to May 2, New York City recorded 32,107 deaths. Laboratories confirmed 13,831 of those were COVID-19 deaths and doctors categorized another 5,048 of them as probable COVID-19 cases. That’s far more deaths than what historically occurred in the city. From 2014 through 2019, the city averaged just 7,935 deaths during that time of year. Yet when taking into account the historical deaths to assume what might occur normally, plus the COVID cases, that still leaves 5,293 deaths not explained in this year’s death toll. Experts believe that most of those deaths could be either directly or indirectly caused by the pandemic.
City health officials reported about 200 at-home deaths per day during the height of the pandemic, compared with a daily average 35 between 2013 and 2017. Again, experts believe that excess is presumably caused either directly or indirectly by the pandemic.
And nationally, a recent analysis of obituaries by the Health Care Cost Institute found that, for April, the number of deaths in the U.S. was running about 12% higher than the average from 2014 through 2019.
Over the last couple months, countless individuals have casted doubts on the accuracy of reporting including Fox News pundit, Tucker Carlson, who questioned the death rate during an April broadcast.
Skeptics site examples of people dying of a heart-attack but inaccurately listed as a COVID death. When someone has a heart condition and also is positive for the virus, citing the cause of death from heart attack would not accurately depict the impact of COVID, while citing COVID might not fully represent the full story.
For this reason, the excess deaths tally could capture the difference in death rates compared to years without a pandemic; painting a realistic picture of the overall impact. This data also captures cases like Wittner’s, where the usual access to health care was disrupted.
A recent analysis from Well Being Trust, a national public health foundation, predicted as many as 75,000 people might die from suicide, overdose or alcohol abuse, triggered by the uncertainty and unemployment caused by the pandemic.
“People lose their jobs and they lose their sense of purpose and become despondent, and you sometimes see them lose their lives,” said Benjamin Miller, Well Being’s chief strategy officer, citing a 2017 study that found that for every percentage point increase in unemployment, opioid overdose deaths increased 3.6%.
At the same time, hospitals across the nation are seeing a drop-off in non COVID-19 cases. People with life threatening conditions may not be seeking appropriate care due to the fear of hospitals being seen as a breeding ground for the virus. Consequently, individuals with symptoms of heart attacks and strokes are staying home and dying.
Furthermore, experts believe a rise in chronic illness deaths due to them not being treated appropriately during the pandemic. This can be due to hospitals delaying treatment like in Sara’s case, or individuals who have “coronaphobia” and don’t want to obtain the treatment they need in fear of contracting the disease.
“You’re not necessarily going to see the direct effect of poor diabetes management now, but when you start having kidney dysfunction and other problems in 12 to 18 months, that’s the direct result of the pandemic,” says Denver cardiologist Dr. Payal Kohli. “As we’re flattening the curve of the pandemic, we’re actually steepening all these other curves.”
Learning From Hurricane Maria
When Hurricane Maria decimated Puerto Rico in 2017, initially the death toll was set at 64. However, more than a year later, after a study done by George Washington University, they factored that the overall death toll including indirect deaths totaled 2,975. Even another study by Harvard said that the death tolls calculated by excess deaths were far greater, totalling around 4,600.
Following the events, the Trump administration caught a lot of flack for their response. After these numbers have come out, FEMA asked the National Academy of Science to calculate how to calculate the full death toll. While the report comes out later this month, they wonder whether they can utilize these recommendations towards the current situation.
Another thing to consider is the complexity of our current situation; compared to a single event like hurricane Maria, the impact of COVID-19 might last for years once the virus stops spreading and the economy improves.
Effect on our Nation’s Mental Health
Where deaths are obviously the worst adverse effect of pandemics, there are other side-effects – our mental health being mostly affected.
For example, natural disasters in the past have been shown to impose negative psychological impacts on those affected. These can include long periods of grief, loss, stress and anxiety proceeding the events.[1]
During the SARS outbreak, one study showed that almost half of the survivors suffered from PTSD. 25% still suffered from this trauma 30 months later.[2] Those psychological effects were not specific to those infected with SARS. Individuals working in high-risk areas, in quarantine, or those close to someone who contracted the disease were 2-4 times more likely to experience severe PTSD than those with limited exposure.[3]
Outside of PTSD, a pandemic can have significant impacts on other mental illnesses. For those who suffer from OCD, the threat of disease and germs can heighten obsessions and compulsions. Times of high stress can also lead to relapse with chronic anxiety sufferers. One study even showed that loneliness and social isolation are twice as harmful to our physical and mental health as obesity.[4]
Experts believe mental health cases will increase dramatically over the next few months. This increase in psychological disorders will be followed by an increase in substance abuse cases as well. Pre-existing conditions or not, using drugs or drinking alcohol is a popular way people cope with these sudden and increasing life stressors.
When combined with “coronaphobia” and lack of finances due to loss of jobs, this can be a perfect storm for individuals with mental health and those in recovery.
Resources
- CBI – Disaster and its impact on mental health: A narrative review
- Science Direct – Risk factors for chronic post-traumatic stress disorder (PTSD) in SARS survivors
- NCBI – The Psychological Impact of the SARS Epidemic on Hospital Employees in China: Exposure, Risk Perception, and Altruistic Acceptance of Risk





